Detect documentation risks before your next inspection.
CareScribe identifies the narrative gaps and escalation omissions in care notes that trigger compliance red flags strengthening your records before they are reviewed.
Privacy-first • Human-in-the-loop • Designed for real workflows
The Problem: Gaps in Documentation Visibility
In regulated care environments, good care must be clearly reflected in documentation. Many risks arise not from care delivery, but from missing or incomplete narrative records.
- Notes written after visits may miss key details.
- Incidents recorded without clear outcomes or follow-up.
- Changes in condition documented without escalation context.
- Manual reviews that are time-consuming and inconsistent.
A Smarter Documentation Review Layer
CareScribe acts as a support layer during documentation. It reviews notes to surface areas that may require clarification or completion.
- Highlights missing or incomplete narrative sections.
- Surfaces potential inconsistencies in documentation.
- Identifies entries that may require follow-up or clarification.
- Supports more consistent and review-ready records.
How CareScribe Reviews Documentation
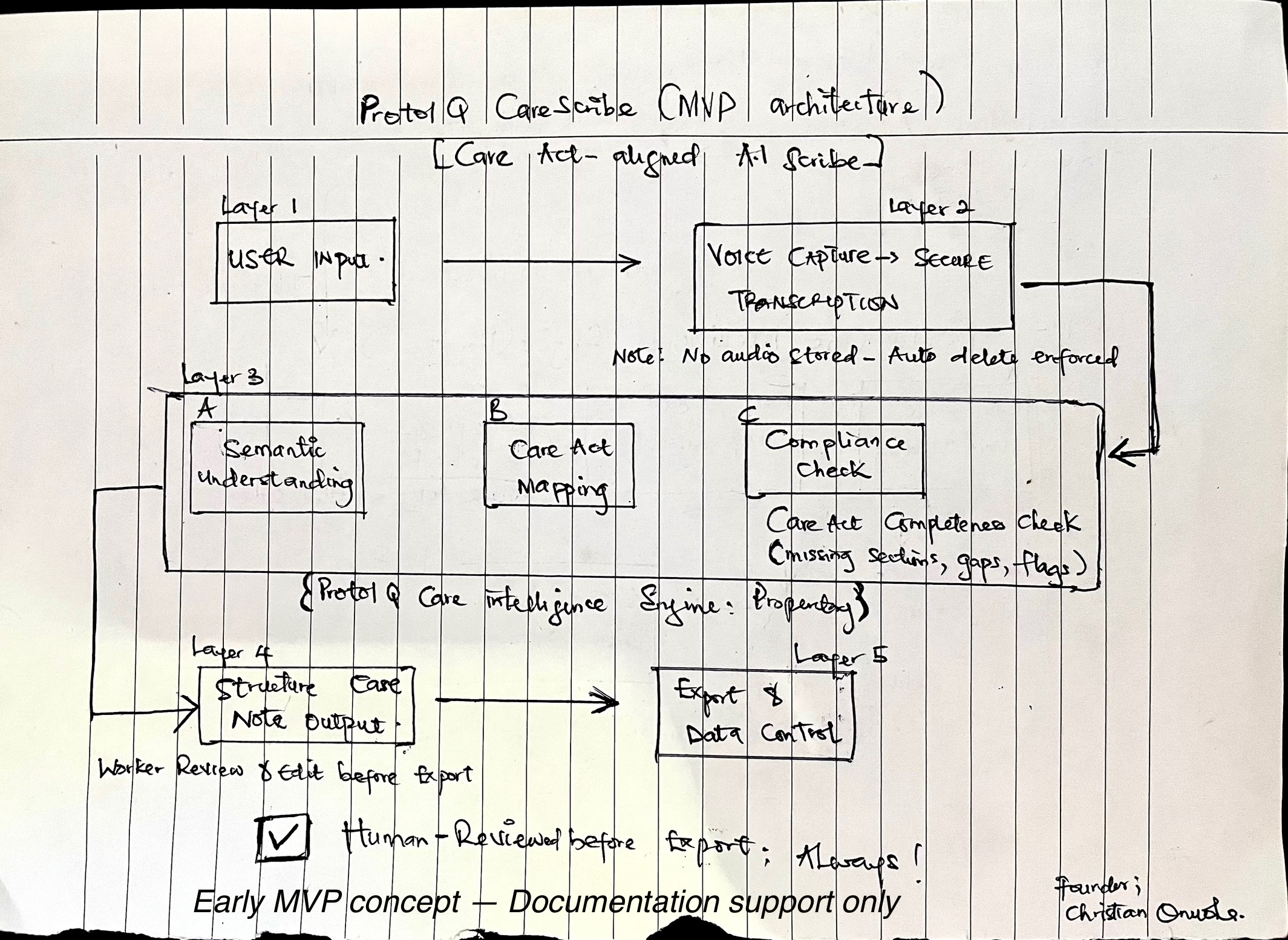
Input → Structured Logic → Risk Detection → Professional Review
Designed for Accountability
✅ What it does
- Highlights documentation gaps
- Surfaces missing context
- Supports review workflows
- Improves narrative consistency
❌ What it does not do
- Replace professional judgment
- Provide clinical decisions
- Guarantee compliance outcomes
- Act without human oversight
In Validation with Care Professionals
CareScribe is currently being refined with input from care professionals to better understand documentation challenges and real-world audit pressures.
Are you a Care Manager or Coordinator? Your expertise can help shape how this system evolves to better support care teams.